

LAB HOURS: MON - THU and SAT : 9:00 AM to 9:00 PM
FRI and SUN : 9:00 AM to 6:00 PM

Article - Emirates Obs-Gyne & Fertility Forum, Volume 02, November 2014
FML at EOFF 2014 in Dubai

Article - Autoimmune Disorders in Gynecology/Obstetrics
PD Dr. med. habil. Michaela Jaksch
Senior Consultant Laboratory, Medicine Medical Director
Freiburg Medical Laboratory ME LLC, Dubai, UAE
Abstract
The spectrum of autoimmune disorders (AD) is broad and can affect almost every organ/tissue. There is increasing evidence that AD are emerging. However, the fact that better laboratory diagnostics with inreased sensitivities are now available, contributes to a significant extent in the recognition of such disorders.
As per the American Autoimmune Related Disease Association (AARDA), 75% of the 50 million Americans affected by AD, are women. AD have been cited in the top ten leading causes of all deaths among US women age 65 and younger (update 2014).
In average, AD affect women 3 times more than men. Eighty different AD are described so far. However around 50% of the 80 described ADs are rare.
Frequent organ specific disorders, such as Hashimoto's disease and diabetes type 1 belong to AD as well as the more rare systemic lupus erythematodes with multi-organ involvement. They all have one in common: the antibodies are directed against the own organ/tissue/cell components.
Several factors influence the predispostion to AD, such as genetic background, environmental and epigenetic factors but also infectious agents.
AD are not in general considered as major cause of primary impaired reproductive capacity, however some AD are associated with significant complications in pregnancy/birth or during implantation.
The immune-endocrine system crosstalk is discussed to play a crucial role, especially in infertility disorders or in the implantation process. In addition, recurrent miscarriages after successfull fertilization and implantation are frequently observed in patients with anti-phospholipid syndrome or in patients with connective tissue disorders.
This short overview will focus on selected AD in the field of Gynecology/Obstetrics and on current strategies in Laboratory Diagnostics.
Autoimmune Disorders in Gynecology/Obstetrics
There are approximately 80 AD based on criteria including breakdown in self-tolerance, demonstrable autoantibodies and/or autoreactive T cells, or infective triggers acting as facilitators in the development of disease (for review see Hayter and Cook 2012).
AD described to affect the pregnancy outcome with impaired implantation, miscarriage or primary ovarian insufficiency (POF) have repeatedly proven to be controversial, and the exact link is still unclear. In addition, many studies are criticised for their retrospective approach.
However, a few disorders seem to play a critical role in implantation, pregnancy and childbirth. In this short overview, I will focus on these disorders.
Antiphospholipid Syndrome (APS)
Five to 15% of women with recurrent miscarriage have clinically significant APS titers, as compared with 2-5% of unselected obstetrical patients (for review see Branch, 2010).
Cervera et al. (2009) performed a 5 years prospective study in 1000 patients (82% with APS). Prematurity and early pregnancy loss were significantly increased (28% and 18% resp.)
Marchetti T. et al. (2013) propose that obstetrical APS is diagnosed when at least one of the following clinical (c) and one of the following laboratory (l) criteria are met:
(c i) 3 or more consecutive abortions before the 10th WOG (maternal anatomical hormonal and chromosomal and paternal chromosomal causes excluded)
(c ii) one or more unexplained deaths of a morphologically normal fetus at or beyond 10th WOG
(c iii) one or more premature births of a morphologically normal neonate before the 34th WOG due to eclampsia or severe pre-eclampsia
(l i) Lupus anticoagulant present in plasma, on two or more occasions at least 12 weeks apart, detected according to the guidelines of the Int. Society on Thrombosis and Hemostasis
(l ii) Anticardiolipin (aCL) antibody of IgG and/or IgM in serum or plasma, present in medium or high titer, on two or more occasions, at least 12 weeks apart, measured by standardized immunoassay
(l iii) significant Anti beta2 glycoprotein of IgG and/or IgM in serum or plasma, on two or more occasions, at least 12 weeks apart, measured by standardized immunoassay
Pathophysiologically, antiphospholipid antibodies are attributed to alter trophoblastic cells including thrombotic mechanisms, inflammation, apoptosis and immunomodulation (Abrahams VM, 2009). Other mechanisms such as damages of other cells by anti phospholipid antibodies, for example endometrial cells, have also been described (D'Ippolito S et al., 2012).
However the detailed pathogenetic mechanisms still remain elusive.
Thyroid Dysfunction due to Auto Antibodies
Thyroid dysfunction and/ or the presence of thyroid autoimmunity (TAI) have both been associated with worse pregnancy outcomes, including miscarriages, recurrent miscarriage, preterm delivery, low birth weight and postpartum thyroiditis in both spontaneous and assisted pregnancies (Thangaratinam et al., 2011; Toulis et al., 2010). A sufficient supply of maternal thyroid hormones is essential for fetal development, especially during the first trimester of pregnancy, when the fetal thyroid gland is not completely functional. The frequent and emerging Hashimoto thyroiditis (around 10% of the population with 90% of females affected) is thought to be significantly involved in thyroid dysfunction and the pathogenesis of hypothyroidism. In a prospective study, Unuane et al. (2013) investigated the prevalence of thyroglobulin (TG) and thyroid peroxidase (TPO) antibodies in women consulting a tertiary referral center for reproductive medicine and found a prevalence of TAI in 16% (163 out of 992 patients). The prevalence of TAI was significantly higher in infertile women as compared to that in fertile controls (19% vs. 13%; p=0.047).
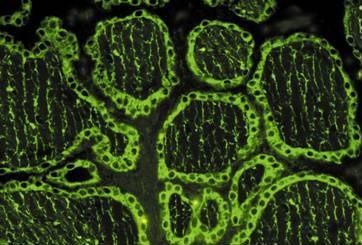
It is recommended to test for TSH, anti TPO antibodies and anti TG antibodies in all cases of fertility impairments (see Fig. 3).
Other Autoimmune Disorders Associated with Pregnancy Complications
Pregnancy and childbirth are known to have profound effect on the disease activity of rheumatic/connective tissue diseases. Adapting the therapy accordingly might be challenging.
High rates of fetal losses are described in SLE women (Andrade et al. 2008).Pregnancy loss, intrauterine growth restriction (IUGR), preterm birth, andpreeclampsia remain major complications in SLE pregnancies.
The pathogenesis of SLE includes significant immune dysfunction. Especially the function of immunosuppression is impaired, including regulatory T-cell function. Regulatory T cells are likely to be the key cell-modulating feto-maternal tolerance (Tower et al., 2013).
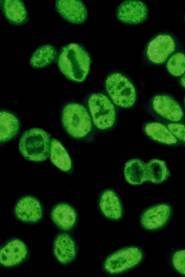
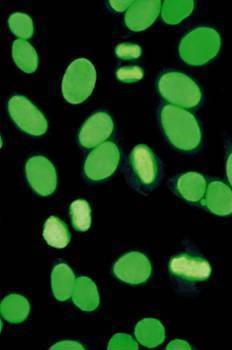
Screening tests for connective tissue disorders such as SLE include anti nuclear antibody (ANA) immunofluorescence (IFT) screening (see Fig. 1 and 2), anti double strand desoxyribonucleic acid (dsDNA) immunoassay and the testing of other autoantibodies using the ANA profile immunoassay. Specific autoantibodies for SLE are nucleosome antibodies, dsDNA antibodies (see Fig. 2) and Sm antibodies. SS-A antibodies (see Fig. 1) are often found in SLE patients. Antibodies to ribonucleoprotein are associated with mixed connective tissue disease (MCTD). Antiphospholipid antibodies should be always tested in these patients as well.
A recent study showed a significant prevalence of antibodies in SLE patients including anti sperm antibodies, anti zona pellucida antibodies and antiphospholipid antibodies when compared to controls. (Ulcova-Gallova et al., 2012).
Celiac Disease
Celiac disease is a mucosal disorder of the small intestine that is related to gluten exposure in genetically predisposed individuals. Symptoms include diarrhea, malabsorption and weight loss. Frequently vitamin B12 deficiency and iron deficiency are observed in these patients.
Impaired fertility and adverse pregnancy outcomes have been described, however reports are controversial and the pathogenesis (immune mediated? nutrient deficiency?) is unclear (Freeman HJ, 2010).
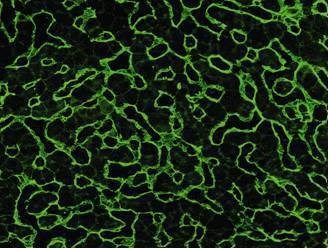
We recommend to test for gliadin and endomysium antibodies (see Fig. 4) as well as for tissue transglutaminase antibodies. Sensitivity and specificity almost reach that of the golden standard (biopsy) with >97% each (several publications).
Anti-Ro/SSA Antibodies
Anti-Ro/SSA antibodies (see Fig. 1) are associated with neonatal lupus (congenital heart block (CHB).
Ro/SSA belong to the group of immunogenic ribonucleoproteins (RNP), involved in cellular RNA transcription, translation, in RNA trafficking and many more processes . Antibodies against Ro/SSA are found in different connective tissue disorders, especially in Sjoegren Syndrome and in SLE.
The gestational outcome is usually not affected when treated appropriately.
CHB is defined as an atrioventricular block diagnosed in utero, at birth or within the neonatal period.
The prevalence of CHB in anti Ro/SSA antibodies positive women is around 1-2%. Overall complete CHB is rare (1:20000 live births) and CHB due to anti Ro/SSA antibodies is considered very rare.
The pathogenesis of neonatal lupus is not clear. Fetal myocarditis, apoptotic mechanisms, genetic predisposition or direct arrhythmogenic effects are discussed (for review see Brucato A et al, 2011).
In summary, autoimmune disorders should be considered as possible causes of adverse effects in fertility, implantation, during pregnancy and at birth.
Figures:
|
|
Fig. 1 SS-A antibodies, Immunofluorescence. Hep-2 cells. With kind permission of Euroimmun, Luebeck, Germany |
|
Fig. 2 Double Strand DNA Antibodies, Immunofluorescence. Hep-2 cells. With kind permission of Euroimmun, Luebeck, Germany |
|
Fig. 3 TPO and TG antibodies, Immunofluorescence. Thyroid gland tissue. With kind permission of Euroimmun, Luebeck, Germany |
|
Fig. 4 Endomysium antibodies, Immunofluorescence. Liver tissue. With kind permission of Euroimmun, Luebeck, Germany |
Literature:
Abrahams VM. Mechanisms of antiphospholipid antibody-associated pregnancy complications. Throm Res 2009; 124(5): 521-5
American Autoimmune related Disease Association (AARDA), http://www.aarda.org/
Andrade R et al. Adverse pregnancy outcomes in women with systemic lupus erythematodes from a multiethnic US cohort: LUMINA (LVI). Clin Exp Rheumatol 2008; 26(2): 268-74
Branch DW. Clinical practise. Recurrent miscarriage. N Engl J Med 2010; 363(18): 1740-7
Cervera R et al. Morbidity and mortality in the antiphospholipid syndrome during a 5-year period: a multicentre prospective study of 1000 patients. Ann Rheum Dis 2009; 68(9): 1428-32
Freeman HJ. Reproductive changes associated with celiac disease. World J Gastroenterol 2010; 16(46): 5810-4
D'Ippolito S et al. Effect of Low Molecular Weight Heparins (LMWHs) on antiphospolipid (aPL)- mediated inhibition of endometrial angiogenesis. PLoS One 2012; 7(1): e29660
Hayter SM and Cook MC. Updated assessment of the prevalence, spectrum and case definition of autoimmune disease. Autoimmun Rev 2012; 11(10): 754-65
Marchetti T et al. Obstetrical antiphospholipid syndrome: from pathogenesis to the clinical and therapeutic implications. Clin Dev Immunol 2013; 2013:159124
Ostensen M and Clowse M. Pathogenesis of pregnancy complications in systemic lupus erythematodes. Curr Opin Rheumatol 2013; 25(5): 591-6
Thangaratinam S et al. Association between thyroid autoantibodies and miscarriage and preterm birth: meta-analysis of evidence. BMJ 2011; 342:d2616
Toulis KA et al. Risk of spontaneous miscarriage in euthyroid women with thyroid autoimmunity undergoing IVF: a meta-analysis. Eur J Endocrinol 2010; 162(4): 643-52
Tower C et al. Regulatory T cells in systemic lupus erythematosus and pregnancy. Am J Reprod Immunol 2013; 69(6): 588-95
Ulcova-Gallova Z et al. Screening tests of reproductive immunology in systemic lupus erythematodes. Autoimmune Dis (2012); 2012:812138
Unuane D et al. Thyroglobulin autoantibodies: is there any added value in the detection of thyroid autoimmunity in women consulting for fertility treatment? Thyroid 2013; 23(8): 1022-8
Accreditation

Accredited according to DIN EN ISO 15189
Our Partners






Lab hours
MON - THU and SAT 9:00 AM to 9:00 PM | FRI and SUN : 9:00 AM to 6:00 PM

Key Technical Personnel
Copyright © 2026 All rights reserved | FREIBURG MEDICAL LABORATORY MIDDLE EAST (L.L.C)